60yr Man with decresed attentiveness
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
A 60year old man came to the hospital with cheif complaints of decreased attentiveness since 3 days and delayed response to verbal stimuli .
He was apparently asymptomatic 1 month back later when he had history if thorn prick to Right lower limb in Harithaharam program on 31st july following which patient visited nearest RMP on 1st August to take some unknown medication and patient developed edema of right lower limb till knee and they went to a hospital in suryapet from there he got referred to Kims for better managment. Here he underwent fasciotomy for Necrotising Fascitis on 4th August and patient was intubated on August 9th till August 15th (for).
When the patient was brought here he has decresed attentiveness since 3 days . He gave delayed response to verbal stimuli.
No h/o vomitings, loose stools, loss of consciousness.
K/c/o Asthma :- used medications for (pt. Attenders dont know)5 months back.(releived)
Not a k/c/o DM, HTN,TB,EPILEPSY,CAD.
He is an occasional alcoholic(--) last binge 1month back.
Blood transfusion done once on 9th august for anaemia(diagnosed at)
He used to work in a rice mill for20yrs till 2010, stopped working there because he had some breathing problem Construction worker till 2years back.





On examination:-
Vitals:- afebrile
Bp-130/80mm hg., PR:- 110bpm, RR:-30cycles/min.SpO2 :-98%at room air , GRBS:- 144gm/dl.
He is a thin built, moderately nourished man with bilateral pedal edema ,pitting type extending till knees with dressings for his wounds to right lower limb.
No sings of pallor, icterus, cyanosis,clubbing.
CVS:- S1 S2 heard. No murmurs
RS:- BAE+, NVBS+, with expiratory wheeze present in both lungs(Rt>Lt).
Per abdomen:-
Soft, non tender, no organomegaly,all hernial orifices are free.
CNS:-
He is conscious,coherent?, cooperative.?
HMF-
Based on his clinical condition the following investigations are ordered
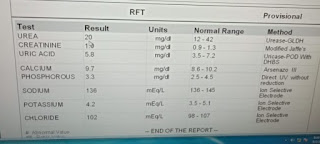
LFT:-



Urinary electrolytes:'
Na+-155 K+--6.5
CBP:-
Serum osmolality :- 259
DAY1:-
TREATMENT GIVEN.:-
1.IVF 3%NaCl @ 10ml/hr
2. IVF.- 2 ampoules of KCL in 0.9%NS over 4hrs
3. Nebulisation with Budecort 12th hrly
SODIUM CORRECTION:-
Sodium deficit:- 0.6xbody weightx(target plasma-starting plasma)
Day2:-
No fresh complaints.
No fever spikes
INVESTIGATIONS:-
1.serum electrolytes


Treatment:'
1.IVF 3% NaCl @10ml/hr(to correct 4-6meq in 24hrs)
2. Syrup.POTCHLOR.15ml in 1glass water TID
3.Nebulisation with Budecort 12th hrly.
4.IVF 0.9%NaCl @ 50ml/hr
5. Tab. OROFER -XT BD
6. Adivised coconut water
Day 3.:'
Patient improved . His response became better compared to day 1( as observed by attenders)
No fever spikes
INVESTIGATIONS:-
Serum electrolytes:-
Na+ 128.,K+ 3.7 ..,Cl- 94
THYROID PROFILE
TSH - 4.06
Treatment:-
1.IVF. 0.9% NS @50ml/hr
2. Syrup. POTCHLOR 15ml in 1glass of water TID
3. Nebulisation with . BUDECORT 12th hrly
4. TAB. OROFER-XT BD
Comments
Post a Comment